
Prof. Dr. Nurullah Ermiş
Skolyoz & Kifoz Cerrahisi
Skolyoz & Kifoz Cerrahisi Nedir?
SKOLYOZ NEDİR? Skolyoz, omurganın yana doğru eğrilmesiyle kendini gösteren ve genellikle "S" veya "C" şeklinde kıvrımlar oluşturan bir durumdur; normalde omurga önden bakıldığında düz bir çizgi oluşturur, ancak skolyozda bu çizgi bozulur ve omurgada belirgin eğrilikler oluşur. Bu durum çoğunlukla çocukluk ve ergenlik döneminde ortaya çıkar ve özellikle büyüme çağındaki bireylerde erken tanı, eğriliğin ilerlemesini önlemek açısından büyük önem taşır.
Skolyozun belirtileri her zaman net olmayabilir. En sık rastlanan işaretler şunlardır: • Omuz veya kalça asimetrisi • Bel veya sırt ağrısı • Göğüs kafesinde hafif eğrilik • Duruş bozukluğu Bu nedenle özellikle çocuklar ve ergenlerde omurga kontrolleri düzenli olarak yapılmalıdır. Erken fark edilen skolyoz, ilerlemenin önlenmesi ve yaşam kalitesinin korunması açısından büyük önem taşır.
Skolyozun nedenleri çeşitlilik gösterir: • İdiopatik skolyoz: En sık görülen türdür, genellikle nedeni bilinmez ve çoğunlukla ergenlik döneminde ortaya çıkar. • Doğuştan (konjenital) skolyoz: Omurganın doğuştan şekil bozukluğu sonucu gelişir. • Nöromüsküler skolyoz: Kas veya sinir sistemi ile ilgili hastalıklar nedeniyle oluşur ve ilerlemesi daha hızlıdır. • Diğer nedenler: Travma, enfeksiyon veya metabolik hastalıklar da omurga eğriliğine yol açabilir. Skolyoz en sık 10–16 yaş arasındaki çocuklarda görülür. Türkiye'de her 100 çocuktan 2–3'ünde klinik olarak anlamlı omurga eğriliği saptanmaktadır. Tanı genellikle fizik muayene ile başlar ve dikim grafisi (full-spine X-ray) ile doğrulanır; gerektiğinde MRI veya CT kullanılabilir.
SKOLYOZ NASIL TEDAVİ EDİLİR? Skolyoz tedavisi, eğriliğin derecesine ve hastanın yaşına göre belirlenir. Hafif vakalarda düzenli egzersiz ve doktor takibi yeterli olabilir. Orta veya ileri derecelerde korse tedavisi uygulanabilir. Eğrilik hızlı ilerliyorsa veya ciddi deformite oluşmuşsa cerrahi müdahale gerekebilir. Prof. Dr. Nurullah Ermiş, skolyoz cerrahisinde Vertebral Body Tethering (VBT) dahil tüm güncel minimal invaziv ve açık cerrahi teknikleri uygular. VBT, büyüme potansiyeli olan adölesan hastalarda omurgayı füzyon yapmadan kademeli olarak düzelten ve hareket kabiliyetini koruyan "büyüme dostu" bir yöntemdir. Büyümesini tamamlamış ya da daha büyük açılı eğriliklerde ise posterior spinal füzyon (PSF), 3 boyutlu navigasyon ve nöromonitörizasyon desteğiyle güvenli ve kalıcı düzeltme sağlar.
KİFOZ NEDİR? Kifoz, halk arasında kamburluk olarak bilinen ve sırt ile göğüs bölgesinde görülen bir omurga eğriliğidir. Yandan bakıldığında baş biraz önde, sırtın üst kısmında ise çıkıntı fark edilir. Kifozun derecesi önemlidir; 20–55 derece arasındaki kamburluk genellikle normal kabul edilir, ancak 55 dereceyi aşan durumlarda tedavi gerekir. Çocuklarda görülen kifoz akciğer ve kalp sağlığını etkileyebilir; ileri yaşta ise nefes alma kapasitesini azaltarak ciddi riskler oluşturabilir. Kifoz doğuştan olabileceği gibi sonradan da gelişebilir. Başlıca sebepler arasında omurganın hasar görmesi veya kırılması, kemik erimesi (osteoporoz), omurga iltihapları, verem hastalığı, duruş bozuklukları ve yetersiz beslenme yer alır.
Kifoz türleri farklı şekillerde görülür: • Doğuştan kifoz: Omurların yapısal kusurları nedeniyle eğrilik oluşur, çocuk büyüdükçe ilerleyebilir. Özellikle hayatın ilk yılında deformasyon hızlı bir şekilde artabilir. • Gelişimsel kifoz: Özellikle 12–15 yaş arasında ortaya çıkar, omurga sertleştiği için eğrilik kalıcıdır. Çocuklarda duruş bozukluğu ve sırt ağrısı sık görülür. • Travmatik kifoz: Kaza veya darbeler sonucu oluşur, ağrı, kas zayıflığı ve bazen sinir sıkışmasına bağlı problemler yaratabilir.
Kifozun en belirgin belirtisi sırtın yuvarlaklaşmasıdır. Diğer belirtiler şunlardır: • Başın vücuda göre önde durması • Boyun, sırt ve bel ağrısı • Omurga sertliği • Nefes darlığı • Bacaklarda güçsüzlük, uyuşma veya karıncalanma • Kaslarda gerginlik • Boyun eğilmesiyle kamburluğun belirginleşmesi • Dik durmakta güçlük
Kifozun derecesine göre tedavi yöntemi belirlenir: • 50–55 derece: Egzersiz ve doğru duruş yeterlidir. • 55–70 derece: Kifoz korsesi kullanılır. • 70 derece üzeri: Cerrahi müdahale gerekir. Ameliyat ile omurlar sabitlenip omurga düzeltilir. Çocuklarda ameliyat sonrası omurgaya yerleştirilen çubuklar, büyümeye bağlı olarak düzenli aralıklarla uzatılır.
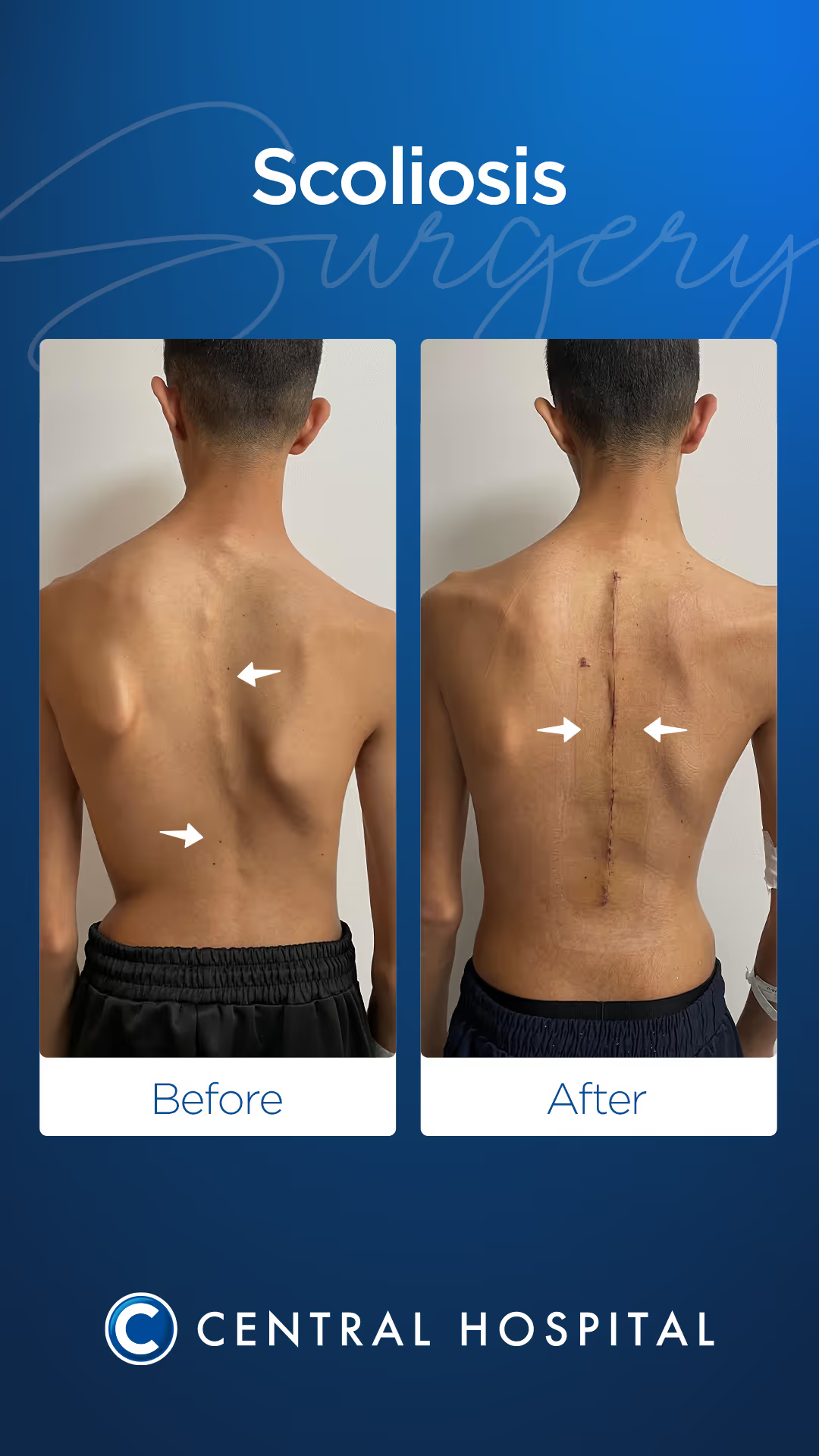
Tedavi Sonuçları
Hastalarımızın Tedavi Sonuçları
Prof. Dr. Ermiş'in gerçekleştirdiği başarılı operasyonlardan derlenen vaka örnekleri.

1 / 4
Belirtiler - Ne Zaman Doktora Gitmelisiniz?
- Sırtta veya belde gözle görülür asimetri ve eğrilik
- Omuzların ya da kalçaların farklı yüksekliklerde durması
- Öne eğilince sırtta belirgin kabarma (jilet sırtı — Adam testi pozitifliği)
- Uzun süre ayakta durmakta ve yürümekte güçlük, çabuk yorulma
- İlerleyen eğrilikle birlikte sırt ve bel ağrısı, kas spazmları
- Ağır vakalarda nefes darlığı, çabuk yorulma ve çarpıntı
- Giysilerin düzgün oturmaması, boy kısalığı hissi
Tedavi Yöntemleri
VBT (Vertebral Body Tethering)
Vertebral Body Tethering (VBT), büyüme potansiyelini koruyan 10–16 yaş arasındaki adölesan skolyoz hastalarında, Cobb açısı 40–65° arasında olduğunda tercih edilen 'büyüme dostu' bir yöntemdir. Ameliyat, göğüs kafesinin yan tarafından yapılan torakoskopik (kapalı, kamera eşliğinde) girişimle gerçekleştirilir; böylece geniş bir kesi yapılmaz ve doku hasarı minimize edilir. Eğriliğin en belirgin olduğu omur seviyelerine titanyum vidalar yerleştirilir ve vidalar arasına yüksek gerilimli esnek polietilen bir bant (tether) gerilerek sistemin kısa eğilim tarafı sıkıştırılır. Hasta büyüdükçe omurga bu bant geriliminin yönlendirmesiyle kademeli biçimde düzelir; füzyon (kaynak) yapılmadığı için omurga hareketliliği ve esnekliği tamamen korunur. Ameliyat sonrası 3–5 günlük hastane yatışı yeterli olup çoğu hasta 4–6 hafta içinde okul ve günlük yaşama döner. Uzun dönem takip çalışmaları, uygun endikasyonlu hastalarda VBT ile %80'in üzerinde birincil düzeltme başarısı elde edildiğini ortaya koymaktadır.
Posterior Spinal Füzyon (PSF)
Posterior Spinal Füzyon (PSF), büyümesini tamamlamış veya Cobb açısı 65° üzerinde olan hastalarda, nöromüsküler ya da konjenital skolyoz gibi ileri vakalarda uygulanan altın standart cerrahi yöntemdir. Sırtın arka tarafından yapılan girişimde, 3 boyutlu bilgisayar destekli navigasyon sistemi ve sürekli nöromonitörizasyon (IOM) eşliğinde eğriliğe dahil her omura pedikül vidaları yerleştirilir. Vidalar, titanyum çubuklar yardımıyla birbirine bağlanır ve omurga eğriliği sagital (yan) ve koronal (ön-arka) düzlemlerin her ikisinde birden düzeltilir. İleri vakalar için posterior yaklaşımın yanı sıra ön yaklaşım (anterior release) da gerekebilir. Ameliyat sonrası hastane yatışı genellikle 3–5 gündür; doğru rehabilitasyon programıyla hastalar 3–6 ay içinde normal yaşam aktivitelerine döner ve çoğu ağır fiziksel iş dışında tüm günlük etkinliklerini gerçekleştirebilir hale gelir.
Ameliyat Öncesi Planlama ve Cerrahi Güvenlik
Skolyoz ameliyatında başarılı sonuç büyük ölçüde ameliyat öncesi planlamanın kalitesine bağlıdır. Eğriliğin tipi, vertebra seviyeleri, omurga dengesi, nörolojik risk, solunum kapasitesi ve kemik kalitesi ayrıntılı olarak incelenir. Ameliyat sırasında nöromonitörizasyon, 3 boyutlu görüntüleme, modern implant sistemleri ve gerektiğinde kan yönetimi protokolleri kullanılarak hem güvenlik hem de düzeltme kalitesi artırılır. Bu yaklaşım, omuriliğin korunmasına yardımcı olurken omurganın kontrollü ve dengeli biçimde düzeltilmesini sağlar.
İyileşme Süreci ve Uzun Dönem Takip
Skolyoz ameliyatı sonrası ilk günlerde ağrı kontrolü, akciğer egzersizleri, erken mobilizasyon ve yürüyüş eğitimi tedavinin ayrılmaz parçalarıdır. Çoğu hasta ameliyattan sonraki ilk birkaç gün içinde ayağa kaldırılır ve taburculuk sonrası aşamalı bir yürüme programı uygulanır. Okula dönüş çoğu zaman 4–6 hafta içinde mümkün olurken, spora dönüş cerrahi tekniğe ve kaynama sürecine bağlı olarak 4 aydan 12 aya kadar değişebilir. Uzun dönem takipte radyografik kontroller, omurga dengesi, implantların durumu ve hastanın fonksiyonel iyileşmesi düzenli olarak değerlendirilir.
Sıkça Sorulan Sorular
Skolyoz ameliyat olmadan geçer mi?
25° altındaki hafif eğrilikler büyüme tamamlandıktan sonra duraksayabilir ve belirli bir kısmı kendiliğinden kısmi düzelme gösterir. 25–45° arası vakalarda korse (spinal ortez) aktif büyüme döneminde ilerlemeyi yavaşlatır; ancak eğriliği kalıcı olarak düzeltemez. 45° ve üzerindeki eğrilikler büyüme sürecinde genellikle hızla ilerlemeye devam ettiğinden ve yetişkinlikte de ilerleyebildiğinden, cerrahi bu olgularda tek etkili ve kalıcı tedavi seçeneği olarak öne çıkmaktadır.
Skolyoz ameliyatından sonra spora dönülebilir mi?
VBT sonrası kademeli spora dönüş genellikle 6–9 ay içinde sağlanır; yüzme ve bisiklet en erken başlanabilen sporlardır, temas sporları ve ağır yüklenme gerektiren aktiviteler için 12 aya kadar beklenmesi önerilir. Füzyon ameliyatı sonrasında ise süreç biraz daha uzundur: hafif-orta aktiviteler 6–12 ayda mümkün olurken, temas sporlarına ve yoğun fiziksel aktivitelere dönüş için genellikle 12–18 ay beklenir.
Skolyoz ameliyatı kaç yaşında yapılır?
VBT büyüme plakaları (fizis) açık olan ve Risser skalası 0–2 arasında bulunan 10–16 yaş grubunda tercih edilir. PSF ise hem adölesan hem de yetişkin döneminde uygulanabilir; yetişkin dejeneratif skolyozunda da ağrı ve yaşam kalitesi bozukluğu belirgin olan hastalarda cerrahi etkili sonuçlar vermektedir. Her hastanın eğrilik derecesi, büyüme durumu ve genel sağlık profili göz önünde bulundurularak bireysel tedavi planı oluşturulur.
Kifoz cerrahisi skolyoz cerrahisinden farklı mıdır?
Kifoz (öne kamburluk), özellikle Scheuermann hastalığına bağlı olgularda veya posttravmatik vakalarda 70–75° üzerine çıktığında cerrahi gerektirebilir. Posterior enstrümantasyon ve füzyon temel yöntemdir; bazı olgularda ön taraf serbest bırakma (anterior release) da eklenir. Hem skolyoz hem de kifoz cerrahisinde amaç, eğriliği güvenli sınırlar içinde düzeltmek, nörolojik yapıları korumak ve hastanın uzun dönem yaşam kalitesini artırmaktır.
Skolyoz ameliyatı riskli midir?
Skolyoz cerrahisi büyük bir omurga ameliyatıdır; bu nedenle kanama, enfeksiyon, nörolojik yaralanma, implant sorunları, yalancı kaynama ve yetersiz düzeltme gibi riskler teorik olarak mevcuttur. Ancak günümüzde nöromonitörizasyon, navigasyon sistemleri, modern implantlar, deneyimli anestezi ekipleri ve standartlaştırılmış ameliyat sonrası bakım protokolleri sayesinde bu riskler geçmişe göre belirgin şekilde azaltılmıştır. Yine de her hastanın risk profili eğriliğin tipi, yaş, eşlik eden hastalıklar ve planlanan cerrahi seviyelere göre bireysel olarak değerlendirilmelidir.
Skolyoz ameliyatı sonrası okul ve günlük yaşama dönüş ne zaman olur?
Hastaların büyük bölümü ameliyattan sonraki birkaç gün içinde yürüyebilir hale gelir ve çoğu 3–5 gün içinde taburcu edilir. Masa başı düzenine veya okul ortamına dönüş çoğu hastada 4–6 hafta içinde mümkün olur; ancak ağır çanta taşıma, uzun süre sabit oturma ve ani dönme-bükülme hareketleri ilk dönemde kontrollü biçimde sınırlandırılır. Günlük yaşama dönüş hızı yapılan ameliyatın kapsamına, ağrı kontrolüne, kas gücüne ve rehabilitasyon uyumuna göre değişir.
Skolyoz & Kifoz Cerrahisi için randevu alın
Prof. Dr. Ermiş ile uzman değerlendirmesi için hemen iletişime geçin.